

Shared Medical Appointment (SMA)
Reimbursement, Revenue, Financial Modeling
The SMA Business Case: How to build the financial model that earns institutional support and keeps your program running.
Why Financial Fluency Matters for SMA Leaders
The clinical case for SMA, also called Group Medical Visits (GMV), is well established. The harder challenge is getting your institution to act on it. Even the most compelling clinical vision requires a credible financial story that is built with rigor, realistic assumptions, and language that administrators recognize. Without it, promising SMA programs stall at the pilot stage or never launch at all.
The challenge is that translating clinical work into financial language (e.g., revenue streams, expense modeling, break-even analysis, multi-year projections) is unfamiliar territory for most clinicians. Meanwhile, administrators evaluating your proposal will expect rigor, specificity, and realistic assumptions.
This page walks you through a four-step framework for building a complete SMA business case, starting with a definition of the problem you are trying to solve all the way to projecting three-year growth of your SMA program. It's written to be accessible whether you're encountering a pro forma for the first time or reviewing financial models regularly.
A critical note before you begin: All billing practices described here must be reviewed and approved by your organization's billing compliance team before implementation. CPT code applicability, payer coverage policies, and reimbursement rates vary by geography, payer mix, and practice setting.

Step 1: Define the Problem and Position SMA as the Solution
Every compelling business case begins not with a solution, but with a clearly defined problem. Resources are allocated to address organizational pain points, so your job is to connect SMA programming directly to problems your institution already recognizes and prioritizes.
Your business case narrative should answer four questions with specificity:
1
What high-priority system problems are you addressing?
Ground your answer in data your institution tracks, such as readmission rates, emergency department utilization for chronic conditions, gaps in chronic disease quality metrics (e.g., HbA1c control, blood pressure management, etc.), provider burnout scores, or access bottlenecks. The more you can anchor your proposal to existing organizational priorities, the stronger your case will be.
2
How are SMA meaningfully different from the status quo?
A standard 15-minute office visit leaves little room for education, behavioral support, or peer connection. SMA programming extends the time patients spend with their care team, incorporate allied health professionals who rarely have billing pathways in traditional visits (e.g., Health and Wellness Coaches), and create group dynamics that improve self-efficacy and adherence in ways that individual encounters often cannot replicate. Be specific about what your SMA model includes that current care does not.
3
Why are SMA the right investment among competing options?
Administrators will reasonably ask why SMA should be implemented rather than expanded individual visit access, a telehealth initiative, or a chronic disease management program. Your answer should speak to efficiency: a billing provider seeing 5-15 patients in a 90-minute SMA spends roughly the same time seeing only 3–4 patients individually, while generating significantly more reimbursement. SMA also create a platform for additional billable services that are difficult to integrate into traditional visit structures.
4
How will you measure success?
Define your metrics in advance across three domains:
Clinical outcomes (e.g., HbA1c, blood pressure, weight, medication dosage)
Healthcare utilization outcomes (e.g., ED visits, hospitalizations, specialist referrals)
Financial outcomes (e.g., revenue per session, cost per patient, net margin)
Committing to measurement upfront signals credibility to administrators and positions your program for quality incentive payments.

With your problem definition and success metrics in place, the next step is mapping exactly where your revenue will come from.
Step 2: Map Your SMA-Related Revenue Streams
The most important financial piece of an SMA program’s puzzle is of course an SMA. Because multiple patients can be billed within a single SMA, the group session itself generates considerably more revenue per unit of time than a clinic with only 1-on-1 visits.
The financial strength of an SMA program can be amplified by coordinating multiple reimbursable services to the SMA programming. For example, an SMA-focused clinical programming can then extend the patient care journey into Medical Nutrition Therapy or Group Psychotherapy sessions, depending on your clinical team’s priorities and staffing.
Understanding which services are available to you, and which CPT codes govern them, is the foundation of your revenue model. The table below organizes the most commonly utilized billable services for chronic disease care by category. Not every service will be available at your institution immediately, but many may already exist in your health system and simply need to be coordinated into your SMA program’s structure.
For clinicians new to billing: CPT (Current Procedural Terminology) codes are standardized codes that tell insurers what service was provided. Each code has an associated reimbursement rate set annually by the Centers for Medicare and Medicaid Services (CMS). Private insurers typically pay at or above Medicare rates.
One-On-One Medical Visits
(99213/99214/99215)
Longitudinal Care
(G2211)
Shared Medical Appointments
(99213/99214)
Health and Wellness Coaching
(99490/99487/99491)
Chronic Care Management
(99487/99490/99491)
Collaborative Care Management
(99492/99493/99494)
Remote Patient Monitoring
(99091/99453/99454/99457/99458)
Intensive Cardiac Rehab
(G0422/G0423)
Medical Nutrition Therapy
(97802/97803)
Group Psychotherapy
(90853)
Group Dietician Visits
(97804)
Exercise Physiology
(97110)
Once you know your revenue streams, the next step is building the full financial picture (i.e., revenue and expenses together) in a structured P&L.
Step 3: Build Your Profit & Loss (P&L) Statement

What Is a P&L Statement?
A Profit and Loss (P&L) statement is simply a structured list of all the money coming in (revenue) and all the money going out (expenses) for your program. Subtract expenses from revenue and you have your "bottom line." A positive “bottom line” means the program pays for itself and generates surplus; a negative one means it requires an investment from your clinic or health system. P&L statements can reflect a single month, a quarter, or a year.
For administrators, the P&L is the primary tool for evaluating program viability and comparing investment alternatives. The key discipline in building a credible P&L is being comprehensive on both sides of the ledger. It is far better to include a line item and estimate it at zero than to omit a cost that later surprises your stakeholders and makes your “bottom line” less favorable or, worse yet, flip from positive to negative.
Revenue Side: Key Inputs
To project annual revenue for each billable service, you need three key numbers that can be used to calculate the revenue from each:
Volume: The number of patients per session multiplied by how many sessions are run annually
CPT code mix: Which CPT codes apply to your patient population (e.g., SMA at 20% 99214 and 80% 99213)
Reimbursement rate: What your payers actually reimburse for each code (your billing team can pull this from your contractual fee schedules to give you the most accurate data for your P&L). If the revenue you are generating is not from reimbursement (e.g., out-of-pocket payment for Health and Wellness Coaching), consider the charge for each visit as the reimbursement rate.
For each revenue-generating service, calculate the annual revenue projection by multiplying volume and reimbursement rate, with consideration of the CPT code mix (as applicable).
As a practical starting point, many SMA programs use a blended CPT code mix for initial projections, then refine as actual billing data becomes available.
Expense Side: What to Include
A common mistake in SMA business cases is underestimating expenses or omitting categories entirely, including:
Personnel Costs (Salary + Fringe/Benefits)
Billing provider time (hours in SMA + documentation time, at applicable compensation rate or opportunity cost of displaced individual visits)
Dietitian or other allied health professional
Care coordinator / medical assistant
Administrative support (scheduling, reminders, consent management)
Overhead and Materials
Conference room or group space reservation cost (or allocated overhead rate)
Equipment (e.g., blood pressure cuffs, scales, etc.)
Printed materials, patient workbooks, educational handouts
Program Development and Training
Staff training in group facilitation
Curriculum development
Marketing and patient recruitment (flyers, portal outreach, staff time)
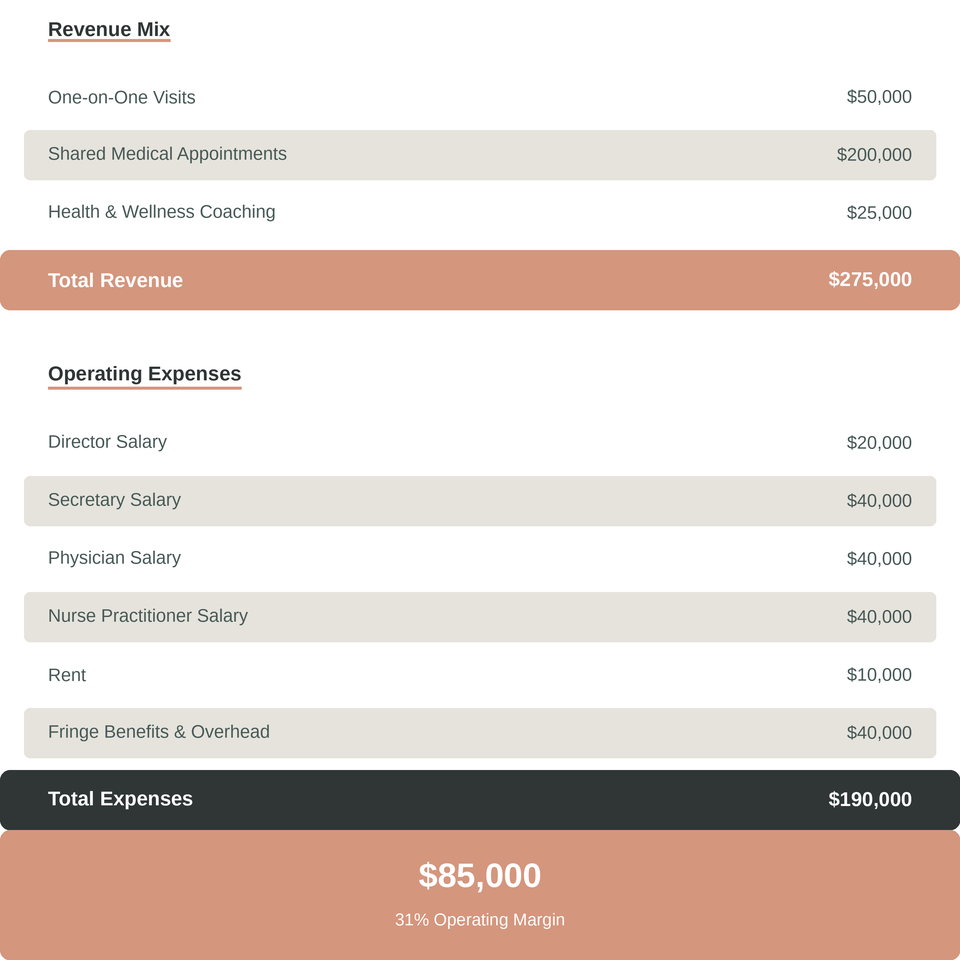
Sample P&L
After developing your P&L for your current program, it’s time to developing a financial growth plan that demonstrates financial sustainability.
Step 4: Project Growth with a Three-Year Pro Forma
What Is a Pro Forma?
A "pro forma" is simply a P&L projected several years into the future. It shows administrators not just where you are today, but where you are going. Because SMA programs typically take 6–12 months to reach steady-state enrollment, the pro forma is essential for demonstrating that a program requiring early investment will become financially self-sustaining over time.
A three-year pro forma should capture three growth levers simultaneously:
Volume growth: Patient census per session increases as referral pathways mature and word-of-mouth builds.
Service expansion: Additional CPT codes become available as your team adds capabilities (e.g., credentialing a dietitian, launching a CCM program, or adding RPM infrastructure).
Session frequency: Moving from monthly to bi-weekly or weekly sessions multiplies revenue without proportional expense increases, since fixed costs (i.e., of your team’s time and resources) are already absorbed.
Key Assumptions to Document
Every pro forma is only as credible as its assumptions. For each of your projections, document the rationale clearly. Administrators will scrutinize your assumptions — having defensible answers to "why did you assume 10 patients per session by month 9?" or "what is your basis for the CCM enrollment rate?" will significantly strengthen your case.
Critical assumptions to address:
Patient recruitment pathway and expected conversion rate from referral to enrollment
Payer mix (Medicare / Medicaid / commercial) and blended reimbursement rates
Billing provider compensation model (employed salary vs. wRVU-based vs. private practice)
Timeline to full enrollment and steady-state operations
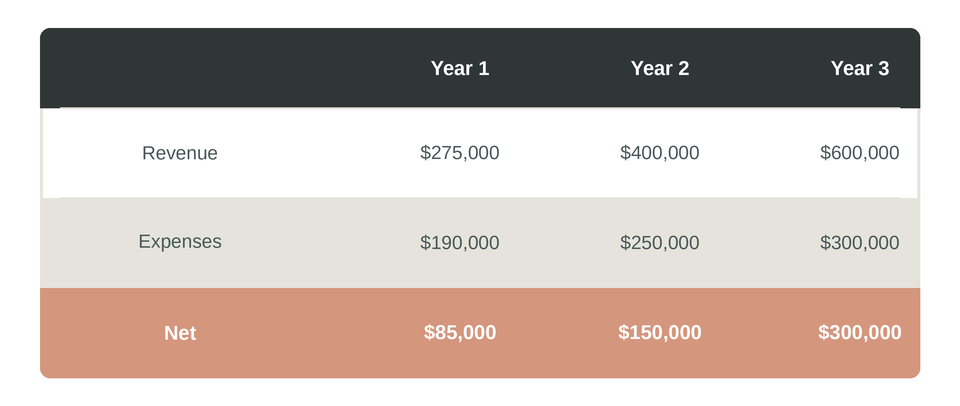
Sample Pro Forma
Putting It All Together
The four-step framework above — problem definition, revenue mapping, P&L modeling, and pro forma projection — gives you the complete architecture of a business case that can win institutional support and sustain your SMA program beyond a pilot.
The most common mistake SMA champions make is leading with clinical evidence and clinical passion, then treating the financial model as an afterthought. Administrators operate in a world of competing capital priorities and finite resources. A rigorous, transparent financial model signals that you understand their world and that you have done the work to make investing in your program a sound decision.
The clinical mission and the financial model are not in tension. A financially sustainable SMA program is one that can serve more patients, improve health outcomes, and retain more providers. The business case is the bridge that gets you there.
All CPT codes, reimbursement rates, and billing guidance on this page are provided for educational purposes. Rates shown reflect approximate 2024 Medicare national payment amounts and will vary by geography, payer, and contract. Always consult your Billing Compliance team before implementing any billing practice.