

Shared Medical Appointment (SMA)
Implementation Guide
Everything your team needs to implement an impactful SMA care model, from session structure and billing and reimbursement to patient recruitment and launch checklists. Built on 30+ years of research and Dr. Jacob Mirsky's 7+ years of real-world SMA implementation experience.
Whether you're just learning about SMA or refining an existing program, this essential SMA implementation guide covers the most important topics you need to succeed:
SMA Session Structure
SMA Billing And Reimbursement
SMA Patient Recruitment
SMA Implementation Checklist
The guidance on this page reflects best practices from 30+ years of SMA research, combined with Dr. Jacob Mirsky's 7+ years implementing SMA at Massachusetts General Hospital / Harvard Medical School and consulting with 20+ clinical organizations.
Please note: These recommendations are intended as general guidance only and do not constitute operational, billing compliance, or legal advice. Always review your SMA plans with qualified billing compliance and legal colleagues before proceeding.
For SMA research studies and additional free SMA implementation resources, go to the Resources page.
Shared Medical Appointment: Structure

There Are Two Halves To An SMA
Every SMA follows the same fundamental structure: two halves that work together to deliver both group-based and individualized care. Session length will vary with patient volume — typically 60 minutes for 5–10 patients and up to 120 minutes for larger groups. Here are the two critical components of an SMA session:
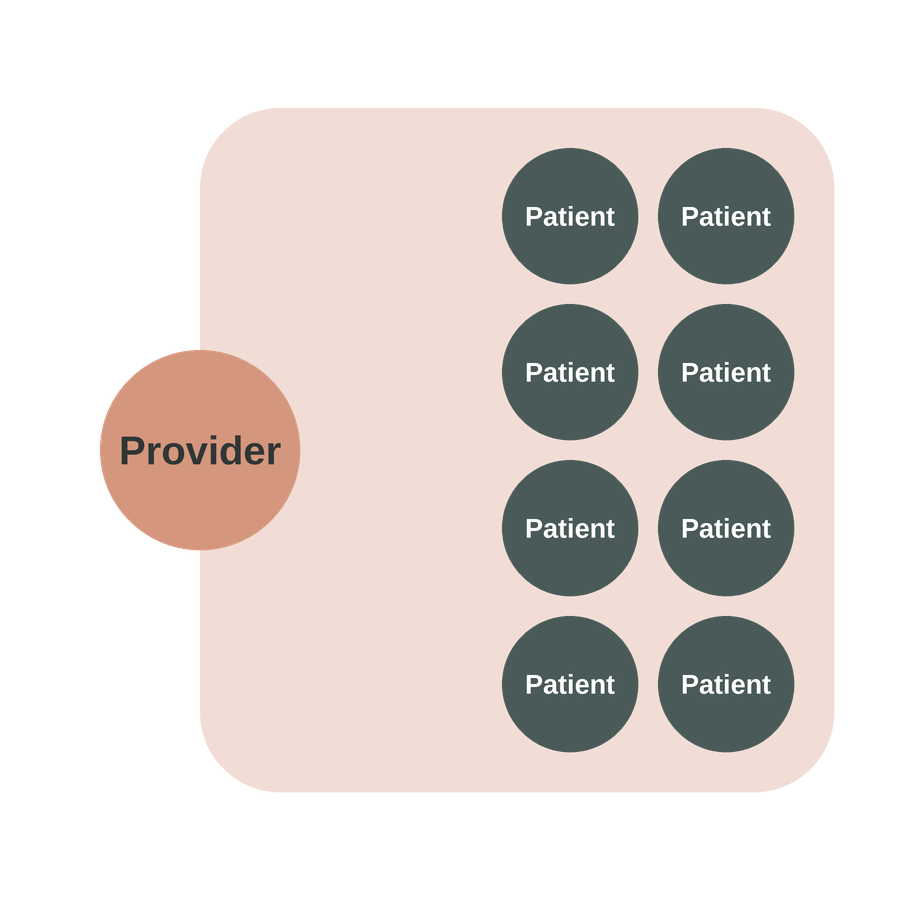
1. Group Education and Shared Experience
In the first half, all patients participate together. This portion typically delivers high-yield information that is too time-consuming to cover in a standard 1-on-1 visit (see Content). Common educational topics include:
Chronic disease basics (e.g., “What is the connection between sodium and blood pressure?”)
Clinical guidelines (e.g., “What is the recommended sodium limit for hypertension?”)
Strategies for behavior change (e.g., “How can you reduce sodium intake in the next week?”)
Other possibilities for group-based care in the first half of an SMA include meditation and mindfulness, culinary medicine, and exercise.
IMPORTANT: the group-based care is not billed to insurance because no individualized care is conducted, as clarified by Medicare.
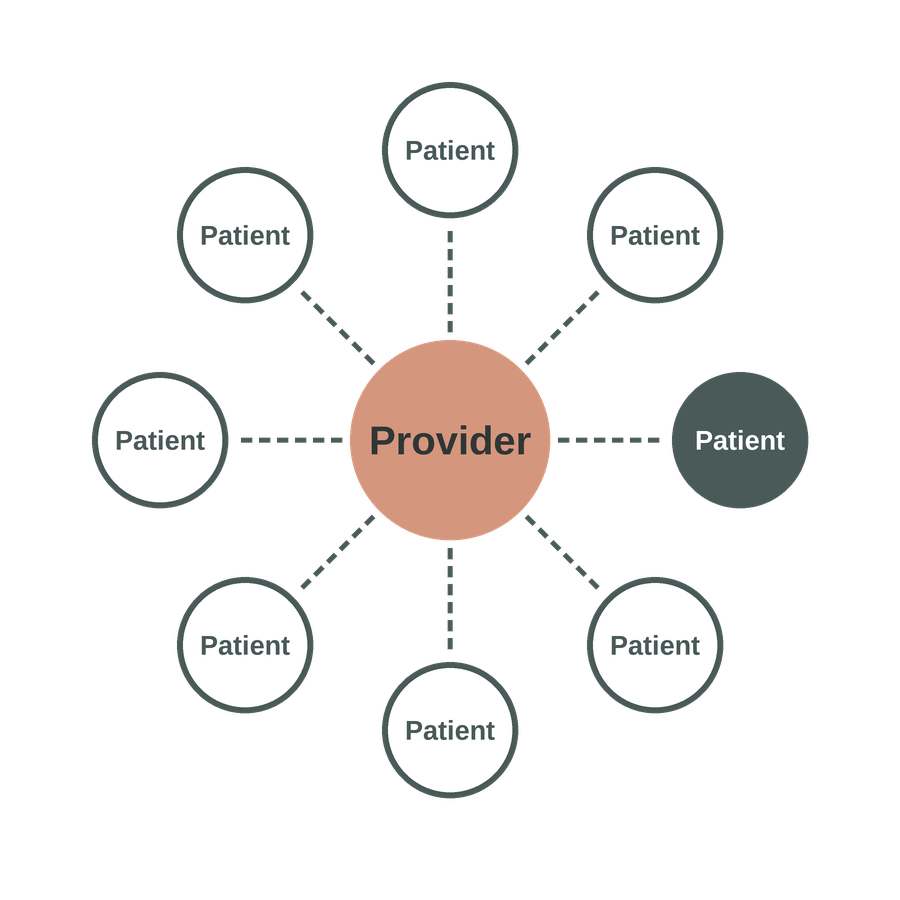
2. Individual Check-Ins
In the second half, each patient has an individualized conversation with the billing provider. Standard Evaluation and Management (E/M) CPT codes for 1-on-1 care are typically used for SMA billing (see below), so it is essential that individualized care occurs within the group context. This can include:
Behavior change treatment of chronic condition
Lab review
Medication management
Do Check-Ins Need to be Private? There are no national guidelines or CPT code specifications regarding whether SMA individual check-ins must take place privately or within the group setting. However, Medicare has indicated that, "there is no prohibition on group members observing while a physician provides a service to another beneficiary." As a result, many SMA providers conduct check-ins within the group so that other patients can benefit from peer sharing and learning, spending a few minutes with each patient before transitioning to the next. That said, it is imperative that you review your SMA workflows with your legal team to ensure patient consent and confidentiality are prioritized.
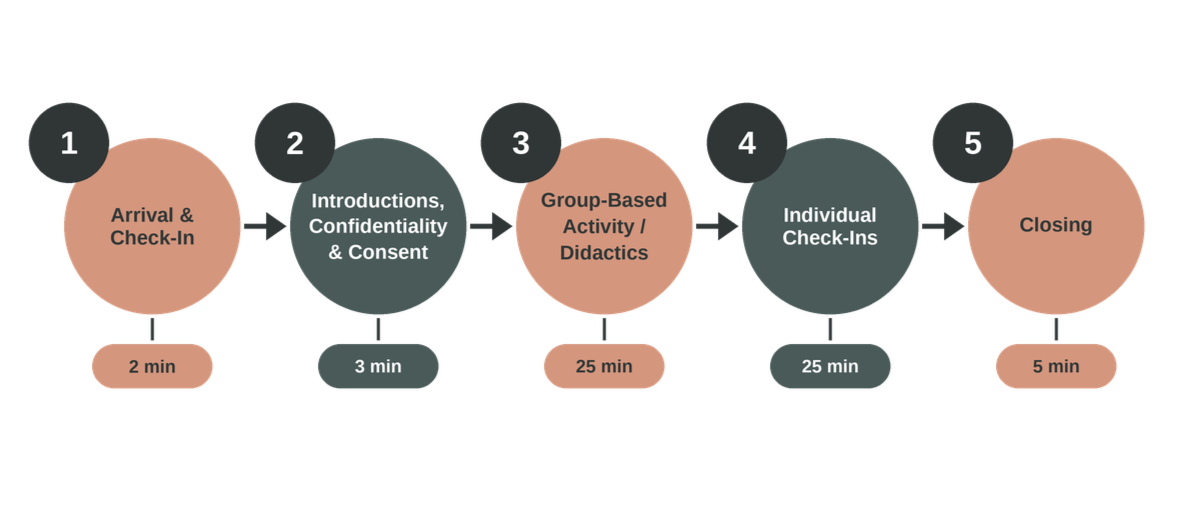
Example SMA Structure
Shared Medical Appointment: Documentation, CPT Codes, Billing and Reimbursement

Before You Bill: What To Do First
Before launching your SMA program, you must confirm with your billing compliance colleagues that the codes you plan to use are approved within your clinic or health system, and that your note templates meet established documentation guidelines. It is best practice to have your billing compliance team communicate directly with insurers to align on expectations before you begin, as suggested by:
American College of Physicians - "ACP recommends that physicians inform each insurer in advance of their intent to begin furnishing group visits and how they plan to bill for them."
American Academy of Family Physicians - "…for compliance purposes, we recommend that you ask for [the payer's] instructions in writing and keep them on file as you would any other advice from a payer."
In short: communicate early, get it in writing, and loop in your billing compliance team before your first session.
There Are No Dedicated SMA Billing Codes
The absence of dedicated SMA billing codes has created significant confusion since SMAs were born in the 1990s. As the American College of Physicians notes: "Because group visits are relatively unusual, no nationally accepted standard has yet emerged for billing them, and there is no special code for standard group visits. Acceptable billing thus varies both geographically and among different carriers. In cases where carriers have yet to adopt policies on group visit billing, the practice may be able to gain acceptance of its own proposed methodology — usually billing for each patient individually based on the services documented in the chart, just as though the patient had been seen separately."
Billing Best Practice: Use Standard CPT E/M Codes 99213 and 99214
Based on guidance from Medicare that, “a physician could furnish a medically necessary face-to-face E/M visit (CPT code 99213 or similar code depending on level of complexity) to a patient that is observed by other patients,” the widely accepted SMA billing best practice is to treat each individual patient check-in during an SMA (see above) as a standard 1-on-1 follow-up visit just as if it took place in a primary care or specialty clinic. As a result, the use of standard CPT Evaluation and Management (E/M) codes 99213 and 99214, which are typically used for primary care and specialty clinic follow-up visits, can be appropriately utilized.
To use these codes in an SMA, you must ensure that:
Every patient receives individualized medical care from the billing provider during the SMA as part of the patient check-in, and
Every note clearly documents Medical Decision Making (MCM) criteria that are needed to bill 1-on-1 follow-up visit (when not billing based on time), as outlined below.
In addition to prior support from Medicare, using standard CPT codes to bill for SMA is supported by the following national organizations:
Moreover, this approach is also supported by publicly available resources from Kaiser Permanente and BlueCross BlueShield of North Carolina.
Because SMA billing practices vary widely, it is imperative that you review your billing approach with your billing compliance team before proceeding.
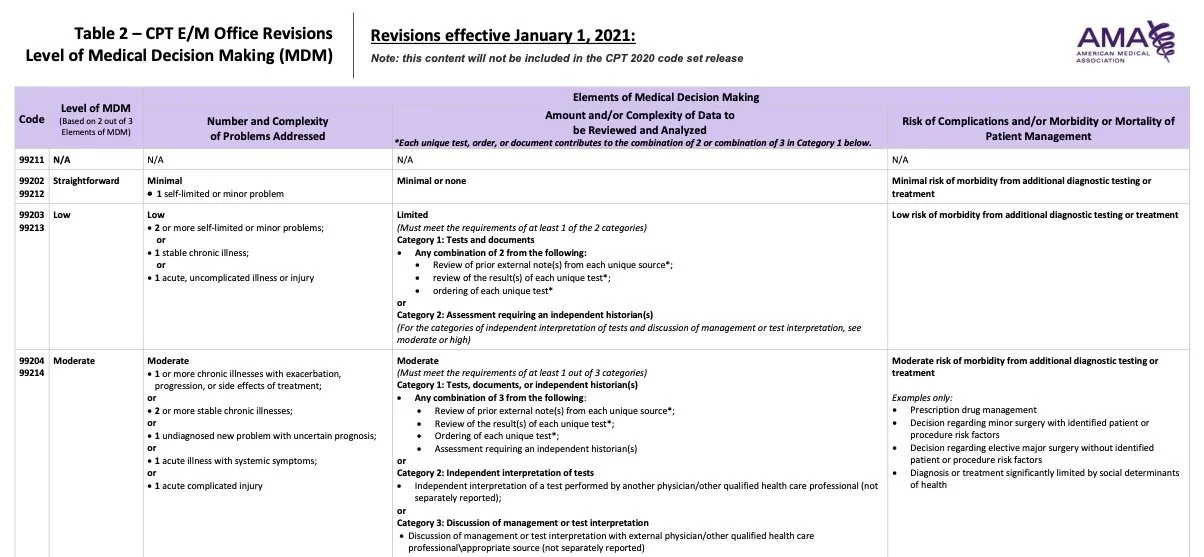
“Medical Decision Making” Criteria For CPT Codes 99213, 99214, and 99215
Unlike 1-on-1 visits, which can be billed based on time, SMA visits can only be billed based on Medical Decision Making (MDM), as defined by the American Medical Association (see table below). These guidelines apply to all insurers, including Medicare and Medicaid, which routinely reimburse for SMA visits.
The MDM table below requires billing providers to achieve 2 out of 3 elements in a billable visit. As a general guide for use in an SMA:
99213 is typically appropriate for SMA check-ins focused on (1) one stable chronic illness with (2) low risk of morbidity from additional diagnostic testing or treatment (e.g., behavior change as the primary intervention).
99214 is typically appropriate for SMA check-ins focused on (1) two or more stable chronic illnesses with (2) either a moderate amount or complexity of data to be reviewed and analyzed (e.g., independent interpretation of tests) or moderate risk of morbidity from additional diagnostic testing or treatment (e.g., prescription drug management).

Shared Medical Appointment: Patient Recruitment

“Definitely the top barrier will be convincing the patients to show up. We invite an average of 10 people and we usually have between 4 and 7 who come and continue to show up. I think patient buy-in is definitely a barrier.”
— SMA Provider (Graham et al., 2021)
How to Fill Your SMA: A Multi-Channel Recruitment Strategy
An effective patient recruitment strategy should employ a broad range of outreach methods to educate both patients and referring providers about SMA programming:
Clinician referrals through the Electronic Medical Record (EMR)
Patient self-scheduling via:
Practice or program website
Social media
Clinic flyers
EMR patient portal messaging
All recruitment materials should clearly communicate that standard billing practices apply to SMA, meaning standard co-payment and deductible charges will be in effect. Patients should also be informed upfront that SMA include group-based care and that they will be asked to consent to sharing personal health information in a group setting.
Patient Scheduling
All patients scheduled for an SMA must be established patients within the practice in order to use the standard follow-up CPT codes (99213, 99214, and 99215). For example:
If your SMA is within Primary Care and you are recruiting exclusively from that panel, no additional steps may be required.
If your SMA is within a specialty clinic such as Cardiology, patients must be established within that specialty practice before enrolling in the SMA.
The scheduling process should therefore include a step to verify that each patient is established in the appropriate practice prior to attending their first SMA session.
Shared Medical Appointment: Implementation Checklist
The Many Facets of SMA Implementation
An SMA is a simple idea that requires thoughtful planning and a commitment to execution. This is why Dr. Jacob Mirsky works with clients to develop SMA Implementation Plans through consulting services that cover a wide range of topics, including:
Organizational readiness - align with leadership, support and sponsorship within the organization, stakeholder meetings
Logistical planning - scheduling, space or virtual capabilities, legal support for confidentiality and consent, billing compliance support for billing and coding
Session structure - clinical program development based on target patient population, session length, group-based content and activity, individual check-ins
Team building - clinical director, SMA leaders, SMA facilitators, administrative leader, scribe, IT support
Team training - group facilitation skills, patient-centered communication, motivational interviewing, behavior change techniques
Patient recruitment - provider referral, self-referral, patient outreach, local advertising, social media
Documentation, Billing, and Coding - note templates emphasizing individualized care (see above), billing and coding standards (see above)
Additional Billing Opportunities - adjunctive billing codes for synergistic clinical services
Key Performance Indicators - patient engagement, clinical outcomes, patient knowledge, behavior change, healthcare utilization, patient and provider satisfaction, financials
Continuous Improvement - team communication, feedback forms, program review, operational changes
Expansion and Scaling - building the business case, financial forecasting
Ready to work through this checklist with an expert? SMA Catalyst's consulting services give you a structured implementation plan tailored to your practice — covering everything from organizational readiness to your first launch. You can also explore the free resources on the Resources page to go deeper on any of these topics.